
.png)
Case Series/Study
Heel wounds pose significant challenges in the healing process due to several factors. The unique anatomy of the heel, including its poor vascularity, limited subcutaneous tissue, and high mechanical stresses during weight-bearing activities, contribute to delayed healing and complications (1).
Split-thickness skin grafts (STSGs) may encounter challenges in healing heel wounds due to specific reasons. The unique characteristics of the heel, such as its thick, callused skin and poor vascularity, contribute to limited graft survival and subsequent failure (2). The mechanical stress exerted on the heel during weight-bearing activities can disrupt the delicate microvasculature of the graft, impeding its integration and viability (3). Additionally, the high incidence of pressure ulcers in the heel region increases the risk of graft breakdown and infection, further compromising healing outcomes (4). These factors highlight the need for alternative approaches. Fish Skin Graft (FSG)* is a novel approach to wound healing. FSG serves to heal into the native tissue upon which it is applied. The purpose of this study is to provide evidence of FSG to adequately provide for lasting heel wound healing.
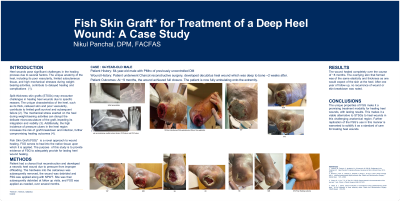
Methods: Patient had a charcot foot reconstruction and developed a necrotic heel wound due to pressure from inadequate offloading. The hardware into the calcaneus was subsequently removed, the wound was debrided and FSG was applied. Site was then subsequently debrided at follow up visits, and FSG was applied as needed, over several months.
Results: The wound healed completely over the course of six months. The overlying skin that formed was the same elasticity and thickened as one would expect of the skin at the heels. After one year of follow up, no recurrence of wound or skin breakdown was noted.
Discussion: The unique properties of FSG make it a promising treatment modality for healing heel wounds, with lasting results. This makes it a viable alternative to STSGs to heal wounds in this challenging anatomical region. Further replication of the FSG’s use in this manner is warranted to solidify it as a standard of care for treating heel wounds.
Trademarked Items:
References: 1. Petrovic, N., Petrovic, V., Ignjatovic, N., & Jovanovic, M. (2019). Challenges in the Treatment of Heel Wounds: A Literature Review. Advances in Skin & Wound Care, 32(1), 39-45.
2. Barnea, Y., Amir, A., Leshem, D., Zaretski, A., Weiss, J., & Gur, E. (2017). Heel coverage with a modified posteromedial thigh perforator flap. Plastic and Reconstructive Surgery - Global Open, 5(7), e1389.
3. Chong, S. J., Lim, T. C., & Tan, B. K. (2019). Current trends in the reconstruction of the heel and sole. Clinics in Plastic Surgery, 46(4), 607-618.
4. Steed, D. L. (2016). Clinical evaluation of recombinant human platelet-derived growth factor for the treatment of lower extremity ulcers. Plastic and Reconstructive Surgery, 138(4S Suppl), 81S-87S.