(CS-043) Treatment of Diabetic Foot Ulcers Using Hydrated, Sterile, Ultra-thick Human Amniotic Membrane Allograft
Introduction: Diabetic foot ulcers (DFU) present a substantial clinical and economic burden to healthcare systems, significantly reducing the quality of life of those affected. Despite aggressive treatment with debridement, infection control, dressings, and offloading, 55% of DFUs fail to heal.1This is alarming as delayed wound healing is the single most common cause of lower extremity amputation among the diabetic population.2-5When DFUs fail to respond to standard of care, skin substitutes and regenerative treatments can be used to support the wound healing process. Ultra-thick human amniotic membrane is one treatment modality that can be used due to its anti-inflammatory and anti-scarring properties, with a key advantage of being readily available without necessitating refrigeration storage.6-8
Methods: A case series of 3 patients with DFUs who were treated with a fully hydrated, sterile, ultra-thick human amniotic membrane derived from the umbilical cord (AM) allograft† in the wound clinic without sharp debridement. In brief, the wound was irrigated, and an AM allograft† was applied without sutures followed by a dressing to maintain moisture control and prevent allograft dislocation.
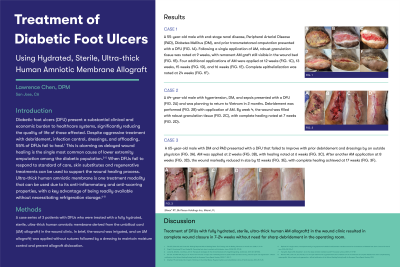
Results: A 55-year-old male with end-stage renal disease, Peripheral Arterial Disease (PAD), Diabetes Mellitus (DM), and prior transmetatarsal amputation presented with a DFU. Following a single application of AM, robust granulation tissue was noted at 9 weeks. Four additional applications of AM with complete epithelialization noted at 24 weeks. Additionally, a 64-year-old male with hypertension, DM, and sepsis was treated with a single application of AM for a DFU; the wound was filled with granulation tissue by week 3, with complete healing at 7 weeks. A 65-year-old male with DM and PAD presented with a DFU that failed to improve with prior debridement and dressings by an outside physician. Following two applications of AM, complete healing was achieved at 17 weeks.
Discussion: Treatment of DFUs with fully hydrated, sterile, ultra-thick human AM allograft† in the wound clinic resulted in complete wound closure in 7-24 weeks without need for sharp debridement in the operating room.
Trademarked Items:
References: 1. Fife CE, Eckert KA and Carter MJ. Publicly Reported Wound Healing Rates: The Fantasy and the Reality. Advances in wound care. 2018; 7: 77-94. 2. Singh N, Armstrong DG and Lipsky BA. Preventing foot ulcers in patients with diabetes. Jama. 2005; 293: 217-28. 3. Jones SA, Scheller J and Rose-John S. Therapeutic strategies for the clinical blockade of IL-6/gp130 signaling. JClinInvest. 2011; 121: 3375-83. 4. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound repair and regeneration: official publication of the Wound Healing Society [and] the European Tissue Repair Society. 2009; 17: 763-71. 5. Sheehan TP and Gondo GC. Impact of limb loss in the United States. Physical medicine and rehabilitation clinics of North America. 2014; 25: 9-28. 6. Raphael A. A single-centre, retrospective study of cryopreserved umbilical cord/amniotic membrane tissue for the treatment of diabetic foot ulcers. Journal of wound care. 2016; 25: S10-s7. 7. Tseng SC, Espana EM, Kawakita T, et al. How does amniotic membrane work? The ocular surface. 2004; 2: 177-87. 8. Marston WA, Lantis JC, 2nd, Wu SC, et al. An open-label trial of cryopreserved human umbilical cord in the treatment of complex diabetic foot ulcers complicated by osteomyelitis. Wound repair and regeneration: official publication of the Wound Healing Society [and] the European Tissue Repair Society. 2019.

.png)