
.png)
Clinical Research
Bacterial infections, which cause tissue damage and inflammation, are a cause of pain for patients with chronic venous leg ulcer wounds. There are no objective, bedside methods for validating patient pain. Therefore, accurately assessing general and localized pain is a challenge for wound care clinicians. We observed in our routine use of bacterial fluorescence (FL) imaging an intriguing co-localization of patient pain with regions of high bacterial loads. This trial was performed to prospectively determine whether local, targeted treatment interventions could reduce pain associated with bacterial loads.
Methods:
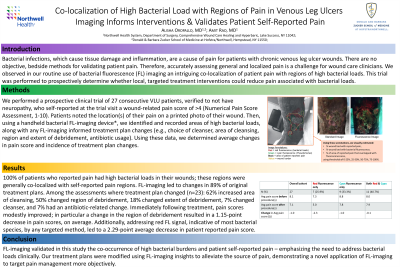
We performed a prospective clinical trial of 27 consecutive VLU patients, verified to not have neuropathy, who self-reported at the trial visit a wound-related pain score of >4 (Numerical Pain Score Assessment, 1-10). Patients noted the location(s) of their pain on a printed photo of their wound. Then, using a handheld bacterial FL-imaging device*, we identified and recorded areas of high bacterial loads, along with any FL-imaging informed treatment plan changes (e.g. choice of cleanser, area of cleansing, region and extent of debridement, antibiotic usage). Using these data, we determined average changes in pain score and incidence of treatment plan changes.
Results:
100% of patients who reported pain had high bacterial loads in their wounds; these regions were generally co-localized with self-reported pain regions. FL-imaging led to changes in 89% of original treatment plans. Among the assessments where treatment plan changed (n=23): 62% increased area of cleansing, 50% changed region of debridement, 18% changed extent of debridement, 7% changed cleanser, and 7% had an antibiotic-related change. Immediately following treatment, pain scores modestly improved; in particular a change in the region of debridement resulted in a 1.15 point decrease in pain scores, on average. Additionally, addressing red FL signal, indicative of most bacterial species, by any targeted method, led to a 2.29 point average decrease in patient reported pain score.
Discussion:
FL-imaging validated in this study the co-occurrence of high bacterial burdens and patient self-reported pain – emphasizing the need to address bacterial loads clinically. Our treatment plans were modified using FL-imaging insights to alleviate the source of pain, demonstrating a novel application of FL-imaging to target pain management more objectively.
Trademarked Items:
References: Flour M, et al. Bacterial colonization in leg ulcers: a clinical and bacteriological survey. International Journal of Dermatology. 2016;55(11): 1257-1264. doi: 10.1111/ijd.13313.
Mani R, et al. A prospective study of pain in venous leg ulcers. Ostomy/Wound Management. 2016;62(12): 34-45.
Woo KY, Sibbald RG. Chronic wound pain: a conceptual model. Adv Skin Wound Care. 2008 Apr;21(4):175-88; quiz 189-90. doi: 10.1097/01.ASW.0000305430.01413.2e. PMID: 18385578.