
.png)
Evidence-Based Practice
During the push-off phase of gait the GRF is shared mainly by the hallux and the first and second metatarsal heads, these structures together taking 64% of the total forefoot load (1). Limited first ray mobility and high pressure at the first metatarsal head are why first metatarsal head ulcerations are most common (2).
An 11-year retrospective review of 59 patients with partial first ray amputation reported an incidence of 42.5% of further amputation. Amputation of the hallux greatly reduces the thrust force during gait, where the hallux with the flexors play a fundamental role, the absence of which was attributed to rise in peak plantar pressures of the first metatarsal stump and lesser metatarsal heads (3). The objective of this study is to present a novel way of addressing first metatarsal head osteomyelitis, to maintain the push off phase of gait and to prevent transfer lesions/ulcerations and ultimately amputations
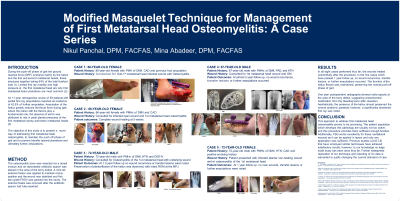
Methods: The osteomyelitic bone was resected via a dorsal incision and an absorbable antibiotic spacer was placed in the area of the bony defect. A mini-rail external fixator was applied medially and the plantar wound was debrided with fish skin graft (FSG)* packed into the cavity. The external fixator was removed after the antibiotic spacer had fully resorbed.
Results: In all five cases, at 1 year follow up, no wound recurrence, transfer lesions, or further amputations occured. The function of the hallux flexors was maintained, preserving the normal push-off phase of gait. One year postoperative radiographs showed radio-opacity at the area of the bony defect, suggesting endochondral ossification from the bleeding bone after resection. Aesthetically, the presence of the hallux almost preserved the normal anatomic parabola, however, a significantly shortened first ray was noted.
Discussion: This approach to address first metatarsal head osteomyelitis proves to be promising. The patient population which develops this pathology are usually not too active, and this procedure provides them sufficient function. Additionally, FSG works excellently for these cavitational wounds as FSG can be applied in layers and only one application was sufficient. Further widespread replication of this technique is warranted to justify changing the standard of care.
Trademarked Items:
References: 1. N. Hayafune, Y. Hayafune, H.AC. Jacob. Pressure and force distribution characteristics under the normal foot during the push-off phase in gait, The Foot, Volume 9, issue 2, 1999, 88-92.
2. Birke JA, Franks BD, Foto JG. first Ray Joint Limitation, Pressure, and Ulceration of the First Metatarsal Head in Diabetes Mellitus. Foot & Ankle International. 1995; 16(5):277-284
3. Borkosky SL, Roukis TS. Incidence of re-amputation following partial first ray amputation associated with diabetes mellitus and peripheral neuropathy: an eleven-year retrospective review. Journal of Foot and Ankle Surgery. 2013, 335-338