(CS-136) Successful Soft Tissue Reconstruction Utilizing Acellular Fish Skin Grafts in a Delayed Ukrainian War Blast Injury
Introduction: Blast wounds significantly contribute to injuries sustained by military personnel and civilians, with nearly 10,000 US occurrences reported from fireworks in 20141. Briefly, blast wounds are categorized as primary (pressure), secondary (fragments), tertiary (structural collapse), and quaternary (thermal)2. There is debate on the temporal nature of contending with soft tissue damage from secondary blast wounds but an agreement that early and frequent debridement is critical3. Outside of trauma-related injuries, the surgeon is often faced with severe tissue loss, which is often highly contaminated and requires the application of novel strategies3. Fish skin graft (FSG) has been tested and considered for battlefield blast wounds with the implications of providing a bacterial barrier and rapid cellular ingrowth4. Therefore, this case aims to evaluate FSG in a secondary blast wound.
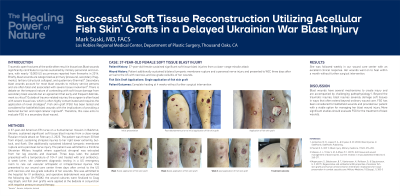
Methods: A 37-year-old American ER nurse on a humanitarian mission in Bakhmut, Ukraine, sustained significant soft tissue blast injuries from a close-range Russian missile attack on February 2, 2023. The patient was thrown 30 feet from impact, sustaining shrapnel injuries to her right lower extremity, buttock, and flank. She additionally sustained bilateral tympanic membrane rupture and a peroneal nerve injury. The patient was admitted to a frontline Ukrainian Military hospital where superficial shrapnel was extracted from her leg wounds and cleansed. Three days later, the patient was presented with a temperature of 104 F and treated with oral antibiotics. A week later, she underwent diagnostic testing in a US ER to rule out vascular orthopedic or intraperitoneal injuries. She presented to our wound care center three days after arrival to the US with necrosis and low-grade cellulitis of her wounds. She was admitted to the hospital for IV antibiotics, and operative debridement was performed the following day. On POD#2, the wound cultures were finalized to Coag neg Staph, and fish skin grafts were applied at the bedside in conjunction with negative pressure wound therapy.
Results: She was followed weekly in our wound care center with an excellent clinical response. Her wounds went on to heal without further surgical intervention.
Discussion: Blast wounds have several mechanisms to create injury and are accompanied by challenging pathophysiology1. Beyond the traumatic injuries, blast injuries severely damage soft tissues in ways that often extend beyond ordinary wound care. FSG has been considered for battlefield wounds and provided our patient with a viable option for managing her blast wound injury. More significant studies should evaluate FSG for the treatment of blast wounds.
References: 1. Jorolemon, M. R., Lopez, R. A., & Krywko, D. M. (2022). Blast Injuries. In StatPearls. StatPearls Publishing. 2. Plurad, D. S. (2011). Blast injury. Military medicine, 176(3), 276-282. 3. Sheean, A. J., Tintle, S. M., & Rhee, P. C. (2015). Soft tissue and wound management of blast injuries. Current reviews in musculoskeletal medicine, 8, 265-271. 4. Magnusson, S., Baldursson, B. T., Kjartansson, H., Rolfsson, O., & Sigurjonsson, G. F. (2017). Regenerative and antibacterial properties of acellular fish skin grafts and human amnion/chorion membrane: implications for tissue preservation in combat casualty care. Military Medicine, 182(suppl_1), 383-388.

.png)