
.png)
Case Series/Study
Diabetic foot ulcers are a serious complication of diabetes that can result in morbidity and mortality. Mortality rates associated with DFU are estimated to be about 5 % in the first year. Diabetic foot ulcers are often difficult to treat particularly when healing has stalled in the inflammatory phase. Kerecis is a FDA approved graft that has been shown to aid in wounds healing. In this study, the purpose was to evaluate the effectiveness of an acellular xenograft, Kerecis, on Diabetic transmetatarsal amputations (TMA).
Methods:
Two clinical case studies of Diabetic TMAs will be presented all utilizing Kerecis, Omega 3 fish skin graft. Patients had all undergone either primary or revisional TMA. We evaluated time to closure as well as number of applications.
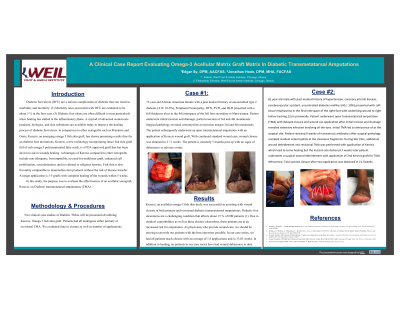
Results: 73yo African American female with a PMH of type 2 diabetes (A1C 10.0%), Neuropathy presents with a full thickness ulcer to the 4th interspace of the left foot secondary to blunt trauma. Patient underwent initial incision and drainage, partial resection of 3rd and 4th metatarsals. Surgical pathology revealed osteomyelitis at resection margin 3rd and 4th metatarsals. Patient subsequently underwent an open TMAwith an application of Kerecis graft. With continued standard wound care, wound closure was obtained in 2.71 weeks. The patient is currently 5 months post op with no signs of dehiscence or adverse events.
61 year old male with PMH CAD, DM2 (A1c: 10%) presented with soft tissue emphysema in the first interspace right foot with underlying wound to right hallux tracking 12cm proximally. Patient underwent open TMA with delayed closure and wound vac application after initial incision and drainage revealed extensive infection involving all the toes. Patient received 6 weeks intravenous antibiotics after surgical pathology revealed residual osteomyelitis at the clearance fragments. Additional wound debridement and revisional TMA was performed with application of graft. 7 weeks later patient underwent a surgical wound debridement with application of 2nd Kerecis graft for TMA dehiscence. Total wound closure after two application was obtained in 21.5 weeks.
Discussion:
Kerecis was successful in assisting with wound closure in both primary and revisional diabetic transmetatarsal amputations. Due to medical comorbidities as well as these chronic ulcerations, these patients are at an increased risk for amputation. In our case series, we had all patients reach closure with an average of 1.6 applications and in 13.03 weeks. In addition to healing, no patients in our case series have had wound dehiscence to date.
Trademarked Items:
References: 1. Pendsey, Sharad P. “Understanding diabetic foot.” International journal of diabetes in developing countries vol. 30,2 (2010): 75-9. doi:10.4103/0973-3930.62596
2. Hughes, O., Rakosi, A., Macquhae, F., Herskovitz, I., Fox, J. and Kirsner, R. (2016). A Review of Cellular and Acellular Matrix Products. Plastic and Reconstructive Surgery, 138, pp.138S-147S.
3. Everett, Estelle, and Nestoras Mathioudakis. “Update on management of diabetic foot ulcers.” Annals of the New York Academy of Sciences vol. 1411,1 (2018): 153-165. doi:10.1111/nyas.13569
4. Tania Woodrow, DPodM MSc,Theresa Chant, BSc RGN, Harvey Chant, BSc MB BS FRCS MD. Journal of Wound Care Vol 28, no 2, February 2019
5. Winters, Christopher DPM, CWS. (2018) Fish Skin to Heal Wounds. Podiatry Management. pp. 119-123.