
.png)
Practice Innovations
Enteric fistulas and ostomies with significant adjacent wounds can challenge patients and providers on multiple fronts. Healing wounds, controlling effluent, and preventing leaks can be frustrating. Furthermore patients with a fistula and a wound may have limited options for discharge and can be bound to a care facility. The employment of fistula isolation devices* (FID) and Negative Pressure Wound Therapy (NPWT) can heal wounds faster and provide a mechanical bolster to prevent loss of dressings and potential leakage.
Methods:
Fistula management requires a team to provide the best quality of life for the patient. Our team follows the S.N.A.P. philosophy: Skin and Sepsis, Nutrition, Anatomy, and planned surgical Procedures.
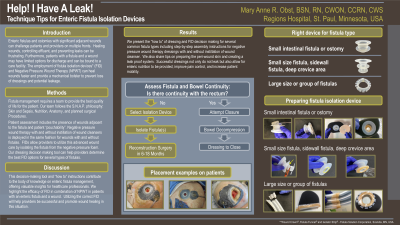
Patient assessment includes the presence of wounds adjacent to the fistula and patient “pouchability”. Negative pressure wound therapy with and without instillation of wound cleansers is deployed in the same fashion for wounds with and without fistulas. FIDs allow providers to utilize this advanced wound care by isolating the fistula from the negative pressure foam. Our dressing decision making tool can help providers determine the best FID options for several types of fistulas.
Results:
We present the “how to” of dressing and FID decision making for several common fistula types including step-by-step assembly instructions for negative pressure wound therapy dressings with and without instillation of wound cleanser. We also share tips on preparing the peri-wound skin and creating a leak proof system. Successful dressings not only do not leak but also allow for enteric nutrition to be provided, improve pain control, and increase patient mobility.
Discussion:
This decision making tool and “how to” instructions contribute to the body of knowledge on enteric fistula management, offering valuable insights for healthcare professionals. We highlight the efficacy of FID in combination of NPWT in patients with an enteric fistula and a wound. Utilizing the correct FID will help providers be successful and promote wound healing in this situation.
Trademarked Items: *WOUND CROWN®, FISTULA FUNNEL®, and ISOLATOR STRIP® (Fistula Solution Corporation, Scandia, MN, 55073.
References: 1. Gribovskaja-Rupp, I. et al. (2016). Enterocutaneous Fistula: Proven Strategies and Updates. Clinics in colon and rectal surgery, 29(2), 130x137. https://doi.org/10.1055/s-0036-1580732
2. Obst, M. A., & Dries, D. (2020). New Compressible Barrier Devices for Enteric Fistula and Ostomy Effluent Isolation. Surgical technology international, 36, 77x 81.
3. Schecter, W. et al. (2009). Enteric Fistulas: principles of management. Journal of the American College of Surgeons, 209(4), 484x491
4. Byrnes MC, Riggle A, Beilman G, Chipman J. A novel technique to skin graft abdominal wall wounds surrounding enterocutaneous fistulas. Surg Infect (Larchmt). 2010;11(6):505-509. doi:10.1089/sur.2010.032
5. https://complexwounds.com/
6. https://www.youtube.com/c/ComplexWoundsandFistulas