Introduction: Patients who develop burns and have underlying diabetes mellitus (DM) are at increased risk for poor outcomes. Patients with DMcan have pre-existing complications including peripheral neuropathy, peripheral vascular disease, and retinopathy.These complications arise withuncontrolled diabetes andplace patients at an increased risk fornon-healing wounds, amputations, and mortalityas a result of their altered physiology.
Methods: A 53y.o.Hispanic male presented to a burn center with a superficial partial thickness burn following the use ofanelectric blanket, after injuring his foot from a staple gun. The patient had type two diabetes mellituswith an A1C of 14.5 on admission andperipheral arterial disease (PAD) that was undiagnosed at admission.Following a split thickness skin graft (STSG) to address the heel burn, the patient developed dusky toes,and eventually underwent amputations of his 2nd through 5thrays.The patient was managed in the outpatient wound care clinic for the toe amputations and developed unstable eschar over his heel skin graft that was not managed by the burn clinic.The wound care clinicutilized aggressive wound care interventions, including sharp debridement and advanced dressingselection.The patient also received additional education regarding management of his DM.
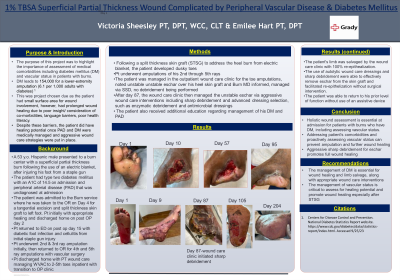
Results: The patient'slimb wasultimately ableto be salvaged by the wound care clinic.The use of autolytic wound care dressings and sharp debridement were able to effectively remove eschar from the skin graft and facilitated re-epithelization.The patient was able to return to his prior level of function and achieved 100% wound re-epithelization.
Discussion: This case highlights the importance of holistic wound assessment at admission for patients with burns who have DM, including assessing vascular status.Education regarding management of DM is essential for wound healing andlimb salvage, along with appropriate wound care interventions.

.png)